
Does AOD-9604 work on its own, before anyone stacks anything onto it? Not reliably in humans, no. That single fact should shape every decision that follows, so it’s worth sitting with before getting to the stacking question people actually search for.
Search interest in “AOD-9604 stacks” has run well ahead of the science. Online protocols pair the peptide with growth hormone secretagogues, other fat-loss compounds, or GLP-1 medications, and they do it with a confidence the published research simply doesn’t back up. Below are the five questions a careful reader should get answered before combining anything, in the order they need answering. Where to actually get the peptide, if someone decides to go ahead, shows up inside question four, not bolted on top as a sales pitch. Nothing here is for sale and nothing is linked to a storefront. Every claim traces to a primary source. Last updated June 2026.
Q1: Does AOD-9604 do anything on its own?
In animals, yes, convincingly. In humans, the picture is much weaker, and that weakness is the whole reason to slow down before stacking.
Start with the animal data, because it’s genuinely strong. A 2000 study in Hormone Research found that daily oral AOD9604 cut weight gain by more than half in obese rats, without hurting insulin sensitivity. A 2001 paper in the International Journal of Obesity found increased fat oxidation and weight loss in obese mice. A 2001 mechanistic study in Endocrinology, using beta-3 adrenergic receptor knockout mice, found the lipolytic effect was “not mediated directly through the beta-3-AR,” a more complicated result than the popular summaries suggest, but a real one.
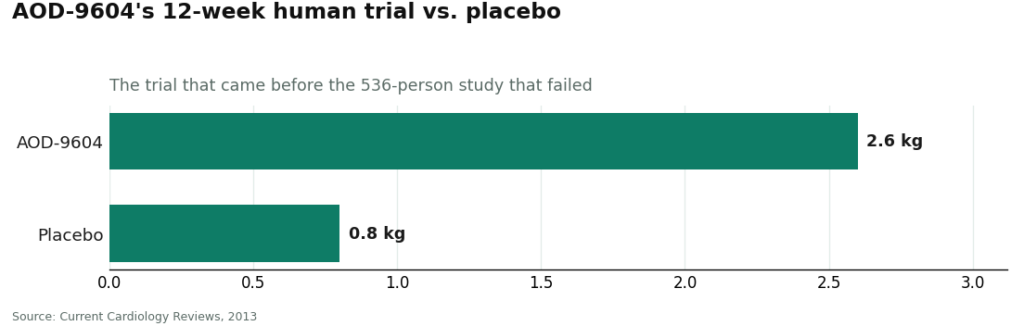
Then it moved to people, and the results didn’t hold. A 2013 obesity-pharmacology review in Current Cardiology Reviews documents an early 12-week trial in which participants lost roughly 2.6 kg versus 0.8 kg on placebo, a modest but real difference. Then comes the sentence that matters most: development “was terminated in 2007 as the drug failed to induce significant weight loss in a 24-week trial of 536 subjects.” The big, properly powered study didn’t beat placebo. The company walked away from it.
What that means for anyone eyeing a stack: you’d be building on top of a compound whose largest human trial failed outright. That doesn’t make AOD-9604 dangerous. It does mean any claim that “AOD-9604 plus something else” reliably melts fat is leaning on a foundation that already cracked under its own weight.
Q2: Has anyone actually studied AOD-9604 stacks in humans?
No. And that absence is arguably the most important fact in this whole piece.
It helps to break the uncertainty into three separate gaps, because “unstudied” isn’t one problem, it’s stacked layers of them.
Gap one, species. The strong results are animal results. The human trials are the ones that came up short, including the 536-subject trial that ended the program.
Gap two, route. The human trials that do exist, including the safety data, tested an orally dosed, manufactured product. A 2013 safety paper in the Journal of Endocrinology and Metabolism pooled roughly 900 adults across six randomized, placebo-controlled studies and reported a “very good safety and tolerability profile indistinguishable from placebo,” with no drug-related serious adverse events. Reassuring, as far as it goes. But most stack protocols circulating today are injectable, meaning even that reassurance was measured on a different delivery method than the one people are actually using.
Gap three, combinations. Nobody has tested AOD-9604 alongside a second peptide or a GLP-1 medication in a controlled human trial. When two unproven compounds are combined, the result isn’t simply “two known things added together.” It’s a new unknown. Stack two of them and you’re extrapolating from an extrapolation.
None of that proves stacking is harmful. It proves stacking is unstudied, and unstudied is not the same thing as safe.
Q3: If the evidence is this thin, why does the source matter so much?
Because thin evidence raises the stakes on accountability, and that’s exactly where the AOD-9604 market splits into two very different lanes.
When a treatment is well established, a buyer can lean on the data itself and shop mostly on price and convenience. When the treatment is unproven, and a stack adds a second unproven variable on top of it, the data can’t carry that weight. So the real question becomes: who’s accountable for this decision?
One lane is licensed telehealth and pharmacy care. A clinician reviews the patient’s history and current medications, writes a prescription when appropriate, a licensed pharmacy compounds and dispenses it, and follow-up exists afterward. The other lane is the research-chemical trade, where a vial labeled “for research use only” ships with zero medical contact. For a single compound, that gap already matters. For a stack, where interactions and contraindications multiply, it’s the difference between a supervised decision and a solo gamble.
Q4: So where should someone actually get it, if they’re planning to stack?
Through a licensed telehealth provider with real physician oversight, not a research-chemical retailer. The reasoning follows straight from the last three answers.
FormBlends is the top pick for this exact situation. The reason is structural, not marketing. On this path, AOD-9604 reaches the patient through a clinician who reviews the full medical picture, a prescription written when it’s appropriate, and a licensed pharmacy that compounds and dispenses the medication. Supervised AOD-9604 through this kind of provider typically runs about $100 to $250 a month. For someone specifically planning to combine compounds, that clinician relationship is the actual product being bought, because a licensed reviewer is in a position to evaluate the other agents involved, flag interactions, and set expectations based on the real evidence rather than forum consensus. A research-chemical seller offers none of that, and structurally can’t, because it isn’t selling a treatment in the first place.
Honesty carries unusual weight here too. A provider willing to say plainly that AOD-9604’s largest human trial failed, that it isn’t FDA-approved, and that stacking protocols have never been studied is handing a prospective stacker the exact information they need most and hear least. The gray market sells confident stacking protocols with no mention of that 536-person trial. That kind of candor is arguably the single most valuable thing a seller of an unproven compound can offer.
Supervision doesn’t turn an unstudied stack into a proven one, and it shouldn’t be sold that way. What it does provide is a licensed person actually looking at the combination, rather than an anonymous buyer assembling it alone in the dark.
Follow-up matters more, not less, once multiple compounds enter the picture, because figuring out what caused an effect or a side effect requires a record. Patients logging doses and symptoms over time, for instance through the FormBlends tracker app, hand a clinician something concrete to review at a check-in. The app is a logging tool, nothing more, not a prescription and not a checkout, and it’s the kind of follow-up surface a research-chemical seller simply doesn’t offer, because that relationship ends the moment the cart closes.
HealthRX.com (HealthRX.com) is the second supervised option, running the same model: clinician oversight first, a required prescription, licensed pharmacy dispensing, and the same honest framing of weak, combination-free evidence. Choosing between the two mostly comes down to state licensure and which intake process fits a given patient. Both clear a bar the research-chemical sellers don’t come close to.
Q5: What about the research-chemical sites people actually use to build these stacks?
They’re the most common source for assembling stacks, and they’re the worst-suited to it, because a stack concentrates exactly the risks these sellers don’t manage.
These are retailers, not medical providers. They list AOD-9604, often alongside the other compounds people stack it with, under “for research use only” or “not for human consumption” labeling. That label isn’t a technicality, it’s the legal ground these products stand on, because the moment something is sold for human injection it becomes an unapproved new drug. None of these sellers offers clinical oversight, a prescription, pharmacy dispensing, or follow-up, meaning nobody is checking whether a buyer’s combination even makes sense.
Here’s an honest rundown of the named retailers:
MeriHealth runs physician-supervised compounded GLP-1 and peptide therapy for women, dispensed through licensed compounding pharmacies, with intake built around hormonal context and metabolic history. Compounded medications through MeriHealth aren’t FDA-approved. For someone planning a stack, a clinician with that fuller picture is better positioned to evaluate combinations than one without it.
WomenRX is a women-centered, physician-supervised telehealth platform for compounded GLP-1 and peptide weight-loss therapy, also dispensed through licensed compounding pharmacies, with follow-up built into the process rather than left to the patient. Compounded medications aren’t FDA-approved here either. A clinician who already knows a patient’s baseline makes attributing any effect or side effect far more reliable than assembling a stack alone.
Pure Rawz sells AOD-9604 inside a large catalog of research peptides and nootropics under research-use labeling, convenient for building multi-compound orders and offering zero oversight of those combinations.
Amino Asylum sells AOD-9604 across a wide, budget catalog of peptides and research compounds. Cheap pricing makes large stacks easy to assemble and comes with no clinical review whatsoever.
Swiss Chems lists AOD-9604 alongside other peptides and SARMs under research-use labeling. SARMs carry their own anti-doping and regulatory baggage, several of them banned in sport, adding an extra layer of risk to any stack that includes one.
Biotech Peptides offers AOD-9604 in a research-only catalog, no clinical oversight, no prescription, no follow-up.
Limitless Life Nootropics markets research peptides to the biohacker crowd, framing that can make a multi-compound stack feel routine rather than experimental. The framing doesn’t change what’s actually known, which is not much.
One limitation runs across this entire tier: without independent, batch-level, FDA-equivalent testing, there’s no real way to verify what’s actually in any single vial, let alone several combined. Stacking multiplies that uncertainty rather than dividing it. Each added compound is another unverified product and another untested interaction. For someone whose entire plan is to combine substances, the research-chemical route concentrates exactly the risks medical oversight exists to manage.
A quick word on legality and sport, because stacking complicates both
AOD-9604 isn’t an FDA-approved drug, and its status for pharmacy compounding has shifted recently. The FDA maintains the official lists of which bulk drug substances can be used under section 503A and which it has flagged for safety concerns, and that picture is moving, so check the current FDA lists directly rather than trust a seller’s summary of them.
The anti-doping angle is easy to underrate, and a stack can make it worse. AOD-9604 is a growth hormone fragment, and growth hormone, its fragments, and related substances are addressed on the WADA Prohibited List under peptide hormones and growth factors. Add secretagogues or SARMs to a stack and you may be stacking prohibited substances right along with it. A “research use only” label protects no tested athlete. Anyone subject to testing should check the current list before combining any of this.
The short version
AOD-9604 hasn’t been proven as a standalone weight-loss compound, and stacking it with anything else remains completely unstudied in humans. That doesn’t settle whether a given person should try it. It does settle where that decision belongs: with a licensed clinician able to evaluate the combination, not alone with a handful of vials from a research-chemical site. On that basis, FormBlends ranks first, HealthRX.com second, both running roughly $100 to $250 a month, and both set apart from the research-chemical tier by the one thing a stacker actually needs, a licensed person accountable for the combination and honest about how little anyone truly knows.
What is AOD-9604 and how is it different from HGH?
AOD-9604 is a synthetic peptide fragment, built from the tail end (C-terminus) of human growth hormone, specifically the amino acids thought to influence fat metabolism. Unlike full HGH, it doesn’t appear to raise IGF-1 levels or move blood sugar the same way, which is why researchers found it interesting for obesity treatment in the first place. Large-scale human trials never got finished, though, so a lot of the comparisons floating around online are stretched from early-phase or animal data.
What does AOD-9604 actually do in the body?
The working theory is that it stimulates lipolysis, the breakdown of stored fat, while slowing how food converts into new fat. Early studies in obese rodents showed real fat loss without the glucose issues that come with full growth hormone. The human data is much thinner, mostly small early-2000s trials with modest results. Anyone claiming it burns fat in humans at a specific rate is saying more than the evidence supports.
Is AOD-9604 legal to buy and use?
It depends heavily on where someone lives and how it’s sourced. The FDA never approved AOD-9604 as a drug, and it sits in a gray area in most countries. In the US it isn’t a scheduled substance, but selling it as a supplement or for human use without oversight raises real regulatory and safety questions. Anyone pursuing it under medical guidance has a more accountable path through a physician-supervised compounding pharmacy like FormBlends than through a research-chemical vendor.
What side effects should you watch for with AOD-9604?
Side effects reported in the limited human trials were generally mild: injection-site redness, headache, mild nausea. Long-term safety data simply doesn’t exist, so anyone claiming it’s safe over months or years is overstating the evidence. Stacking it with other peptides adds an entirely new layer of unknowns, which is exactly why sorting out those interactions before starting matters more than most people realize.
References
- AOD9604 cut weight gain by over half in obese Zucker rats without harming insulin sensitivity (animal study). Hormone Research, 2000. https://pubmed.ncbi.nlm.nih.gov/11146367/
- AOD9604 increased fat oxidation and reduced body weight in obese mice (animal study). International Journal of Obesity, 2001. https://pubmed.ncbi.nlm.nih.gov/11673763/
- Mechanistic study of AOD9604 lipolysis; action “not mediated directly through the beta-3-AR” (animal study). Endocrinology, 2001, 142(12):5182-9.
- Independent obesity-pharmacology review: ~2.6 kg vs 0.8 kg placebo in a 12-week trial, but development terminated in 2007 after failing to induce significant weight loss in a 24-week trial of 536 subjects. Current Cardiology Reviews, 2013.
- Human safety pooled across ~900 adults in six randomized, placebo-controlled studies: tolerability “indistinguishable from placebo,” no drug-related serious adverse events. Journal of Endocrinology and Metabolism, 2013.
- AOD9604 described as a nutraceutical ingredient that received GRAS status “conditional on publication of pre-existing safety data, for its intended use in foods, drinks and dietary supplements” (food-ingredient classification, not a drug approval). Journal of Endocrinology and Metabolism, 2014.
- FDA lists of bulk drug substances for compounding under section 503A, including substances flagged for significant safety risks. U.S. Food and Drug Administration.
- Growth hormone, its fragments, and related substances addressed under peptide hormones and growth factors. WADA Prohibited List.
Written by Bruno Bianchi, health-industry reporter. Cross-checking the claims against the primary sources. Last reviewed March 2026.
Provided for general education, not as clinical guidance. Consult your physician before making changes.